Dr. Tim Flynn, Physical Therapist | Educator | Movement Scientist | International Speaker, is a guest contributor. Dr. Flynn is widely published with over 100 peer-reviewed manuscripts on musculoskeletal disorders and chronic spinal pain. He has received numerous professional awards. He is a world-renowned clinician whose primary clientele includes clients suffering from chronic pain disorders. Tim and Jan Dommerholt have presented a dry needling workshop together at a past APTA-CSM conference.
Dr. Flynn frequently writes about important topics related to physical therapy on his Substack page. With Tim’s permission, we are featuring his Substack blog from April 9, 2026. The blog resonates strongly with Myopain Seminars’ point of view we share with our dry needling students.
For 99% of human history, rotator cuff tears existed. We just hadn’t figured out how to turn them into problems yet.
How many of us have friends or family with shoulder pain? Or perhaps you are suffering from shoulder pain. Folks with shoulder pain frequently seek out answers in the physician’s office, walking in with shoulder pain but leaving with a diagnosis.
“You have a rotator cuff tear.”
It sounds precise.
It sounds explanatory.
It sounds like we’ve found the problem.
But there’s one issue. We may have just taken something normal… and turned it into something that sounds pathological.
The Study That Should Make Us Really Uncomfortable
A recent population-based MRI study published in JAMA Internal Medicine examined the shoulders of healthy, pain-free adults aged 40 to 70—not patients seeking care, but people from the general population.
Then they scanned both shoulders. What they found should fundamentally change how we talk about the shoulder.
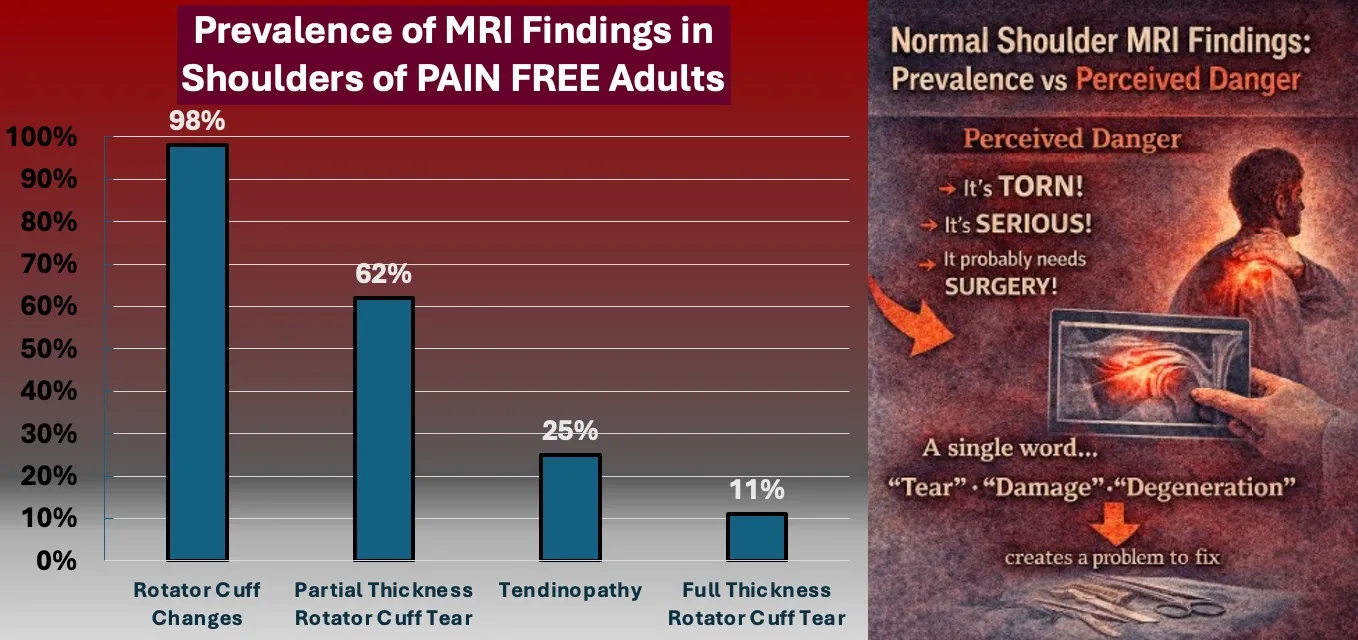
- 98% of people without shoulder pain had rotator cuff abnormalities
- Only ~4% of the shoulders examined were “normal”
- Over 60% of people with no shoulder pain had partial-thickness tears
- Even full-thickness tears were present in people with no pain
Let’s translate that:
If you take a group of people from 40 to 70 years of age with no shoulder pain and scan them,
almost all of them will have something that looks abnormal, and we call it pathology.
The Problem Isn’t the MRI
The MRI is doing exactly what it was designed to do.
It is exquisitely sensitive.
It detects subtle structural variation.
It captures change over time with remarkable precision.
In many ways, it’s one of the most powerful diagnostic tools medicine has ever created. But here’s what’s easy to forget:
For most of human history, we couldn’t see any of this.
For thousands of years, clinicians made decisions based on:
- symptoms
- function
- observation over time
We didn’t know what a “partial-thickness tear” looked like.
We didn’t know what “degeneration” looked like.
We didn’t have the ability to identify every irregularity in human tissue.
And yet…people still got better.
Then Everything Became Visible
In the last few decades, imaging technology has changed the game. Suddenly we could:
- see inside joints
- visualize soft tissue
- identify microscopic changes
- detect structural variation long before symptoms appeared
It felt like progress, and it was. But it came with an unintended consequence:
We started seeing things we didn’t yet understand how to interpret.
Just because you can see something… doesn’t mean it’s the problem.
The New Problem: Too Much Information, Not Enough Context
We now routinely detect and diagnose findings that are:
- common
- age-related
- often asymptomatic
In many cases, they are closer to normal human variation than pathology.
But instead of integrating that context, we often do something much simpler. We name them. And we name them with words like:
- tear
- degeneration
- tendinopathy/tendinitis
- damage
When Visibility Becomes Vulnerability
Here’s the paradox:
The more clearly we can see inside the body, the easier it becomes to overinterpret what we see.
We’ve moved from a world of uncertainty… to a world where everything has a label. And once something has a label, it rarely stays neutral.
It becomes:
- a diagnosis
- an explanation
- a target
The Critical Mistake
We treat imaging findings as if they are causal, when many of them are simply incidental.
That distinction matters. Because when an incidental finding is described as a problem, it doesn’t stay incidental for long.
The Real Issue
The MRI didn’t create the problem. It revealed variation. We created the problem when we:
- removed context
- added implication
- and delivered it with language that suggests something is wrong
The Better Perspective
Imaging is a tool. A powerful one. But like any tool, its impact depends on how it is used—and how it is explained. Because in modern musculoskeletal care, the issue is not that we can see too little.
It’s that we now see so much…that we’ve forgotten how to distinguish:
What matters from what merely exists.
The Language Gap
To a clinician, a “rotator cuff tear” might mean:
- partial thickness
- degenerative
- clinically irrelevant
- expected with age
To a patient, it means:
- ripped
- broken
- unstable
- needs fixing
That gap is not just a communication issue; it’s a clinical issue, as it often leads to riskier, more invasive procedures.
When Normal Becomes a Diagnosis
Here’s the quiet shift that has happened in musculoskeletal care. We’ve moved from:
“These are common changes we see with aging”
to:
“You have a tear”
One is descriptive. The other is declarative.
One normalizes. The other medicalizes.
And once something is labeled as a problem, it tends to behave like one.
The Cascade We Pretend Not to See
It usually goes like this:
Step 1: Shoulder pain
Step 2: MRI
Step 3: “Tear”
Step 4: Concern
Step 5: Referral
Step 6: Intervention
At no point did we stop to ask:
“Is this finding actually the cause of the pain?”
Because once the word is introduced, the story writes itself.
The Shoulder as a Case Study in Overinterpretation
This is not a fringe issue. Shoulder imaging is one of the clearest examples of a broader pattern in medicine:
- Structural findings are common
- Correlation with symptoms is inconsistent
- Language implies causation anyway
We don’t just identify abnormalities. We assign them responsibility.
What If We Changed the Story?
Instead of:
“You have a rotator cuff tear.”
Try:
“These are very common variations we see in the shoulder, especially as we get older. Most people do very well with movement and strengthening.”
Same MRI. Different interpretation. Different behavior. Different outcome.
The Bigger Point
This isn’t about denying pathology. It’s about recognizing that not all structural findings are:
- meaningful
- causal
- actionable
And more importantly: Not all of them need to be named in a way that creates fear.
The Bottom Line
We didn’t just discover pathology. We created it—at least in how it is understood. Because when nearly everyone has “abnormalities,” the abnormal is no longer abnormal. It’s just human.
The real question isn’t:
“What did the MRI show?”
It’s:
“What did we just turn into a problem?”