
Believe it or not, there actually is research regarding clinical pearls. They are considered “small bits of free-standing and self-contained clinically relevant information, based on experience or observation.1 They are derived “from patient-centered observations and should apply to other patients”, which is my hope with this Clinical Pearl.
Sometimes, when treating patients, the most obvious solution may not always be as obvious as it seems. That was the case when I recently treated a 39-year-old male Navy SEAL who was one year status post ACL repair. His surgery went as expected until he developed an infection shortly into his rehab, which delayed his recovery with a fair degree of pain and swelling. He returned to therapy a year out because he continued to have limitations with training and had become frustrated.
His primary complaints were:
- Limited knee extension
- Inability to perform a shallow single-leg squat
- Failure to perform a deep squat and
- Difficulty stabilizing with single-leg stance.
Upon examination, he indeed presented with limited active and passive knee extension due to “tension in the back of the knee.” The common culprits had been examined, including the hamstring and gastrocnemius, as they cross the posterior aspect of the knee. His arthrokinematics had also been examined, including the anterior tibial glide needed for extension and superior patellar motion. Both were unremarkable.
Treatments that had proved beneficial in similar cases were explored, such as grade III oscillations into knee extension, resisted terminal knee extension, and quad-set straight leg raises. Unfortunately, either the patient was unable to execute the activity or the activity did not produce the expected results.

Although some myofascial trigger points were located in the quads, hamstrings, gastrocnemius, and deep rotators of the hip, none reproduced his symptoms or provided relief. Based on the patient’s persistent complaint of posterior knee “discomfort,” one of the last muscles to be examined was the popliteus. The popliteus was found to be exquisitely tender, and because the patient indicated it was “his pain.” It was needled.
Following the needling, the patient immediately demonstrated full active, weight-bearing knee extension. Much to his surprise, he was also able to assume a single-leg standing position and perform a controlled, shallow single-leg squat. He stated the knee felt more stable and then attempted a bilateral squat with upper extremity support. That too was successful.
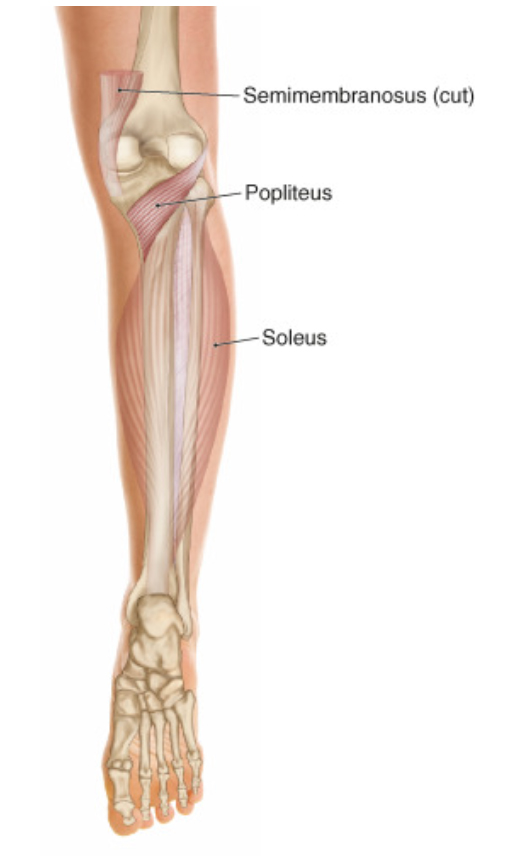
The popliteus might not be an obvious choice with limited knee extension, but since this experience, I have made it a permanent part of my exam. The muscle is a small triangular muscle, originating on the posteromedial tibial cortex and narrowing as it wraps around the posterior knee to insert just anterior and inferior to the FCL (fibular collateral ligament) on the lateral femoral condyle.2 Its primary function is to internally rotate the tibia in relation to the femur in open-chain and stabilization of external rotation of the femur in relation to the tibia in closed-chain situations.2
What is of particular interest regarding the popliteus is that it can increase stiffness with passive knee extension, external rotation, and isometric knee flexion and internal rotation. It also demonstrates increased stiffness when weight-bearing and yet decreased stiffness with the knee slightly flexed during single-leg standing.3
The popliteus may not be first on the list of muscles considered with knee injury, but it is often associated with injuries to the anterior and/or posterior cruciate ligament. It is also frequently injured due to direct trauma to the antero-medial tibia, with external rotation forces while the knee is in hyperextension, and even with downhill running when done with long strides.4,5 The muscle should also be examined for myofascial trigger points following total knee arthroplasty, especially when persistent, limited knee extension is present.
Needling of the popliteus is in our DN3 curriculum. It may be a muscle of concern for some, but it need not be. Dry needling of the popliteus is both safe and accurate.6 Like me, it could be the muscle you are missing because it’s not always apparent. But it is easy to treat, and one I hope you will now consider dry needling the muscle when indicated.
Rob Stanborough, PT, DPT, MHSc, MTC, CMTPT, FAAOMPT | DN Instructor
References
- Lorin MI, Palazzi DL, Turner TL, Ward MA. What is a clinical pearl and what is its role in medical education?. Med Teach. 2008;30(9-10):870-874. doi:10.1080/01421590802144286
- Wood A, Boren M, Dodgen T, Wagner R, Patterson RM. Muscular architecture of the popliteus muscle and the basic science implications. Knee. 2020;27(2):308-314. doi:10.1016/j.knee.2019.12.001
- Yagi M, Tateuchi H, Kuriu M, Ichihashi N. The function of the popliteus muscle: An in vivo ultrasound shear wave elastography study. Hum Mov Sci. 2021;76:102751. doi:10.1016/j.humov.2020.102751
- De-Arriba-Agre JI, García-Mulas C, Grigelmo-Hernández S, et al. Dry Needling of the Popliteus Muscle Validation by Ultrasound Imaging: A Cross-Sectional Observational Study. J Clin Med. 2022;11(21):6409. Published 2022 Oct 29. doi:10.3390/jcm11216409
- Morrissey CD, Knapik DM. Prevalence, Mechanisms, and Return to Sport After Isolated Popliteus Injuries in Athletes: A Systematic Review. Orthop J Sports Med. 2022;10(2):23259671211073617. Published 2022 Feb 28. doi:10.1177/23259671211073617
- Rodríguez-Sanz J, Pérez-Bellmunt A, López-de-Celis C, et al. Accuracy and safety of dry needling placement in the popliteus muscle: A cadaveric study. Int J Clin Pract. 2021;75(11):e14669. doi:10.1111/ijcp.14669