A Severity-Based Framework for Clinical Practice
Dry needling can produce a wide range of patient responses—from brief soreness or minor bleeding to rare but serious complications. Yet clinicians and researchers have lacked a consistent way to describe these responses. Is transient soreness an adverse event? Does brief lightheadedness warrant the same label as syncope? Should every unexpected response be classified as harmful?
A new international Delphi study by Kearns and colleagues addresses this problem by proposing a severity-based framework for classifying unintended responses and adverse events associated with dry needling.
Why terminology matters
Previous dry needling research has used the terms minor, mild, moderate, significant, serious, and major inconsistently. Responses including soreness, bruising, pain, and bleeding have sometimes been classified as adverse events even when they are anticipated, self-limiting, and clinically manageable.
This inconsistency has practical consequences. It makes safety data difficult to compare across studies, complicates patient education and informed consent, and can lead clinicians to document similar events differently.
The new framework shifts the focus away from rigid lists of event types. Instead, it asks clinicians to consider the significance of a response for the individual patient.
How the framework was developed
The researchers invited 100 dry needling experts to participate in a three-round modified Delphi process. Eligibility required at least three years of dry needling practice, five years of clinical experience, and experience in dry needling education or scholarship.
Sixty-five experts completed the first round, and 52 experts from nine countries completed all three rounds. Most participants were physical therapists or physiotherapists. Consensus required at least 80% agreement, a median rating of at least 3 on a four-point scale, and an interquartile range of no more than 1.
The panel reached strong agreement that adverse events should be classified along a spectrum and that severity and functional consequences are more informative than the type of response alone.
Unintended response or adverse event?
A central contribution of the study is its distinction between an unintended response and an adverse event.
An unintended response is a reaction that was not the treatment goal but remains within the range of possible expected clinical outcomes. It does not cause meaningful functional disruption or require escalation of care.
An adverse event is an outcome that exceeds expected clinical outcomes. Its classification depends on the severity of the response, its effect on function, clinical management, and whether referral or additional medical care is required.
This distinction recognizes that the same general type of response may fall into different categories depending on its presentation. For example, brief dizziness with normal vital signs and complete recovery may be an unintended response. Dizziness accompanied by pallor, diaphoresis, and a sustained reduction in blood pressure may constitute an adverse event.
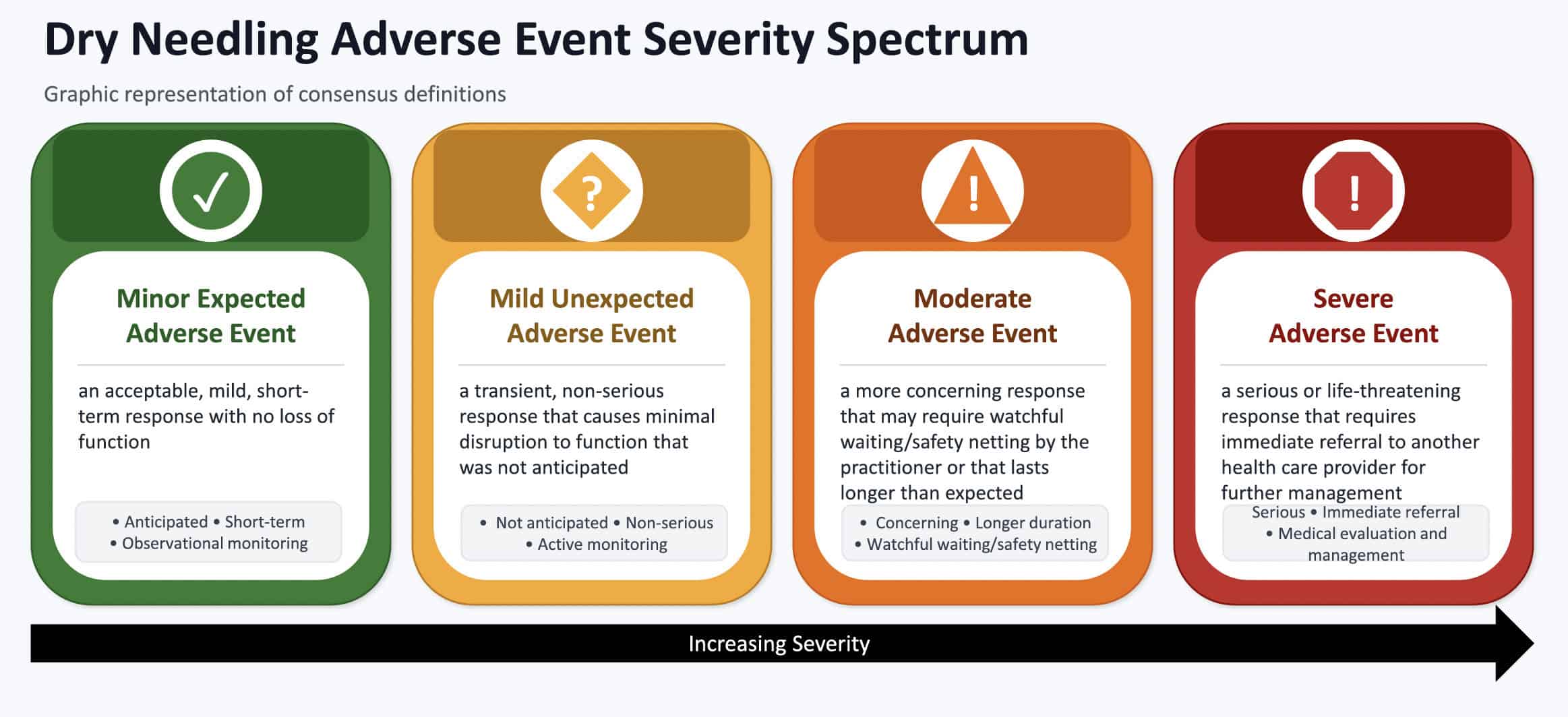
A four-level severity spectrum
The proposed framework classifies adverse events into four categories:
- Minor Expected
The response is clinically anticipated but exceeds what would be considered a neutral unintended response. It may require active monitoring, but causes little or no lasting functional disruption. - Mild Unexpected
The response is not anticipated, produces limited functional impact, and may require self-management or clinician follow-up, but does not require referral to another healthcare provider. - Moderate
The response causes meaningful functional disruption and requires direct clinician intervention, structured monitoring, or safety-netting. The patient does not require emergency evaluation or referral. - Severe
The response requires immediate referral, medical evaluation, or medical management. Examples include pneumothorax, significant peripheral nerve injury, subdural hematoma, or infection.
Importantly, these categories are not determined by diagnosis or symptom type alone. A clinician should consider the entire clinical presentation.
Five questions to guide classification
The study identifies five interacting considerations:
- Was the response expected or unexpected from the clinician’s perspective?
- How long did it last?
- Did it negatively affect the patient’s function?
- What level of clinical management was required?
- Was referral to another healthcare provider necessary?
Duration contributes to the clinical picture, but the expert panel did not support using time alone as an independent criterion for classification. A short-lived response can still be clinically significant, while a longer-lasting response may remain mild if it has little effect on function and requires minimal management.
“Expected” also has a specific meaning in this framework. It refers to whether the treating clinician would reasonably anticipate the response.
Applying the framework in practice
Consider several examples presented in the paper.
A patient experiences mild post-needling soreness that resolves within two hours, does not limit activity, and requires only education and observation. This is classified as an unintended response rather than an adverse event.
During needling near a peripheral nerve, another patient reports brief paresthesia that resolves immediately when the needle is repositioned. Reassessment reveals no sensory or motor deficit. This also falls within the unintended-response category.
By contrast, a new headache that persists into the following day, causes the patient to cancel treatment, and requires an over-the-counter analgesic, may be classified as a Mild Unexpected adverse event.
Syncope requiring direct clinician intervention, repeated assessment of vital signs, and a formal observation period represents a Moderate adverse event when the patient subsequently recovers and can leave independently.
Progressive chest pain and shortness of breath resulting in emergency referral and confirmation of pneumothorax clearly meet the criteria for a Severe adverse event.
These examples show why event labels alone are insufficient. Dizziness, pain, bleeding, or neurologic symptoms cannot be classified reliably without considering objective findings, functional consequences, management, and clinical context.
Implications for dry needlers
For clinicians who perform dry needling, the framework offers a more structured approach to documentation and clinical reasoning. A useful clinical note should record:
- The patient’s subjective response
- Relevant objective findings
- Whether the response was anticipated
- Its duration and progression
- Any effect on activity or participation
- Monitoring or intervention provided
- The need for follow-up, referral, or medical care
This information supports continuity of care and allows later reviewers to understand why a particular classification was chosen.
The framework may also improve patient communication. Rather than describing all possible post-needling reactions as equivalent “risks,” clinicians can explain that responses occur along a continuum. Common, transient reactions can be distinguished from events that may require additional care, while still giving patients clear instructions about symptoms that warrant contacting the clinician or seeking urgent evaluation.
For researchers, shared terminology could improve the comparability of safety findings across studies. Reporting only whether an event occurred provides limited information. Reporting its severity, functional effect, management, and outcome offers a more meaningful account of clinical safety.
Important limitations
This framework is preliminary. It represents expert consensus, not prospective validation, and should not yet be interpreted as a definitive standard of care.
Although the panel included experts from several countries, approximately 69% practiced in the United States, and more than 92% were physical therapists or physiotherapists. The findings may therefore not fully represent other professions, healthcare systems, or regulatory environments.
The framework also depends on clinical judgment. Borderline cases may be classified differently when expectedness, duration, functional impact, and management do not point to the same level. Future research must test inter-rater reliability and determine whether clinicians can apply the categories consistently to standardized cases and real-world events.
A more patient-centered approach to safety
The most important message from this study is that the clinical significance of a dry needling response cannot be determined by its name alone. What matters is how severely the patient is affected, whether function is disrupted, and what must be done to manage the response safely.
By replacing prescriptive event lists with a patient-centered severity spectrum, the proposed framework offers a promising foundation for clearer documentation, more meaningful patient conversations, and more consistent safety reporting. Its ultimate value, however, will depend on prospective testing and reliable application across clinicians and settings.
Based on: Kearns GA, Sheldon A, Barrett T, Puentedura E, Brismée J-M, Dommerholt J. “A severity-based classification framework for dry needling unintended responses and adverse events: An expert consensus Delphi.” Musculoskeletal Science and Practice. 2026;85:103618. https://doi.org/10.1016/j.msksp.2026.103618