Why the Newest Evidence on Dry Needling Should Change How Clinicians Read the Literature—and Choose Their Educators
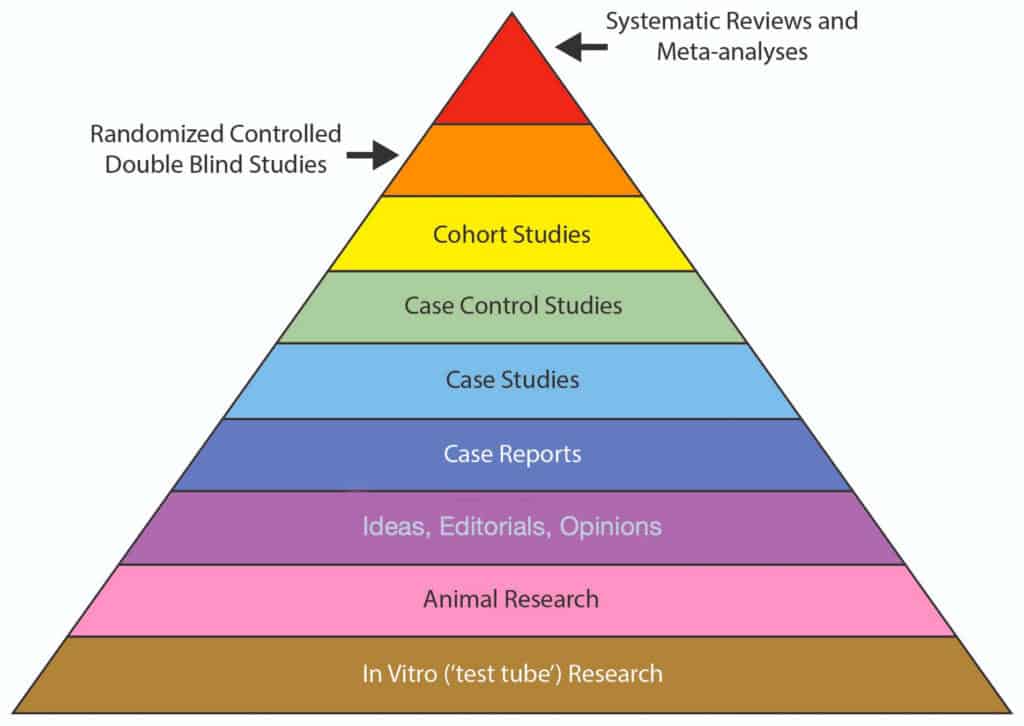
Evidence-based practice rests on a hierarchy of research. At or near the very top of that hierarchy sit systematic reviews and meta-analyses. Clinicians often assume that if a conclusion comes from a systematic review, it must be reliable. A newly published systematic review of systematic reviews challenges that assumption.
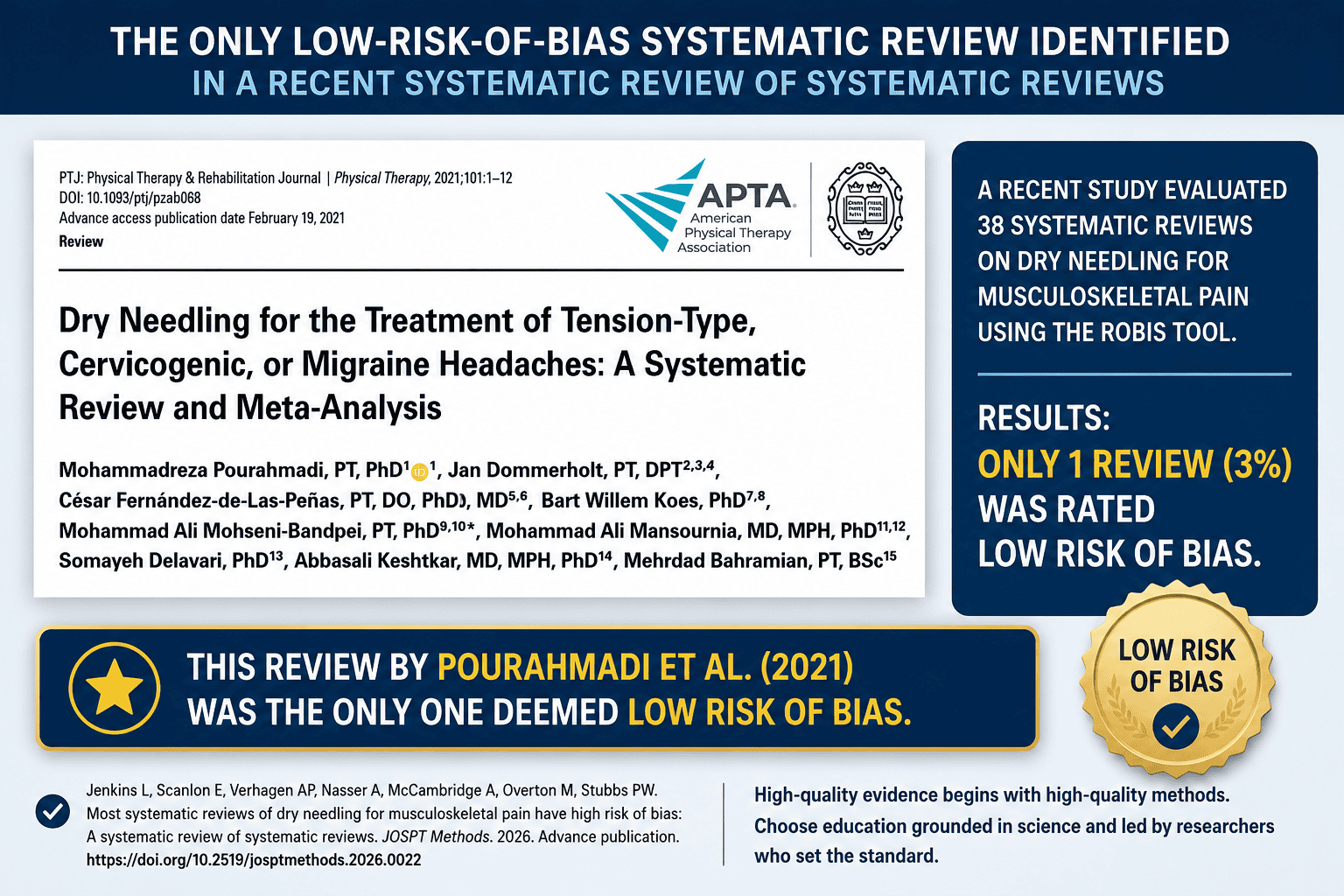
Jenkins and colleagues recently evaluated the risk of bias of systematic reviews investigating dry needling for musculoskeletal pain using the ROBIS (Risk of Bias in Systematic Reviews) assessment tool (1). Rather than asking whether dry needling works, the authors asked a more fundamental question:
How trustworthy are the systematic reviews themselves?
The answer should make every clinician pause.
A Surprising Finding
The authors identified 38 systematic reviews published between 2009 and 2024. After evaluating each review using the internationally recognized ROBIS instrument, they found:
- 31 reviews (82%) had a high risk of bias
- 6 reviews (16%) had an unclear risk of bias
- Only one review (3%) achieved a low risk of bias
This finding reminds us that systematic reviews are not automatically high-quality evidence simply because they summarize multiple studies. Like any scientific publication, they can be affected by methodological weaknesses, including problems with eligibility criteria, literature searches, data extraction, interpretation, and statistical synthesis. As Jenkins et al. conclude, the findings of many systematic reviews “need to be interpreted with caution.”
Why Risk of Bias Matters
Risk of bias is not the same as study quality. A review may appear comprehensive, include many studies, and even perform sophisticated meta-analyses. Yet, if bias is introduced during study selection, appraisal, or synthesis, the resulting conclusions may overestimate—or underestimate—the true effectiveness of an intervention.
This distinction is precisely why Jenkins and colleagues used the ROBIS tool instead of relying solely on methodological quality checklists. Their goal was to determine whether readers could have confidence in the conclusions drawn by existing systematic reviews. For clinicians trying to make evidence-informed decisions, this distinction is critically important.
The One Review That Met the Highest Standard
Among the 38 systematic reviews evaluated, only one received a low-risk-of-bias rating (2).
That review was:
Pourahmadi M, Dommerholt J, Fernández-de-las-Peñas C, Koes BW, Mohseni-Bandpei MA, Mansournia MA, et al. Dry needling for the treatment of tension-type, cervicogenic, or migraine headaches: a systematic review and meta-analysis. Physical Therapy. 2021;101(5).
The paper was conceived by the study’s first authors, Drs. Mohammad Pourahmadi and Jan Dommerholt. The Jenkins review does not claim that this headache review proves dry needling is effective or that all of its conclusions are necessarily correct. Rather, it concludes that, based on ROBIS, its methodology was the only one among the included reviews judged to have a low risk of bias, thereby standing out for methodological rigor. High-quality conclusions begin with high-quality methods.
Pourahmadi and Dommerholt are among the most influential researchers, educators, and clinicians in dry needling, and they have co-authored several studies (3-5). Two new papers are currently under review for publication (6,7). Dommerholt’s contributions extend well beyond publishing original research. They include advancing safety standards, developing educational curricula, mentoring clinicians worldwide, and contributing to systematic reviews that withstand the highest levels of methodological scrutiny.
What This Means for Continuing Education
Today, there are approximately 60 companies in the United States offering dry needling education.
Many advertise similar promises:
- Evidence-based instruction
- Expert faculty
- Comprehensive techniques
- Improved clinical outcomes
Yet the new review highlights an important reality: Not all evidence is created equally. If clinicians are going to invest their time, money, and professional reputation in learning dry needling, they should ask an important question:
Who is teaching the evidence?
More importantly:
Who has demonstrated the ability to produce evidence that withstands the highest standards of scientific evaluation?
In other words, how many instructors of those 60 companies actually contribute to the development of the dry needling field?
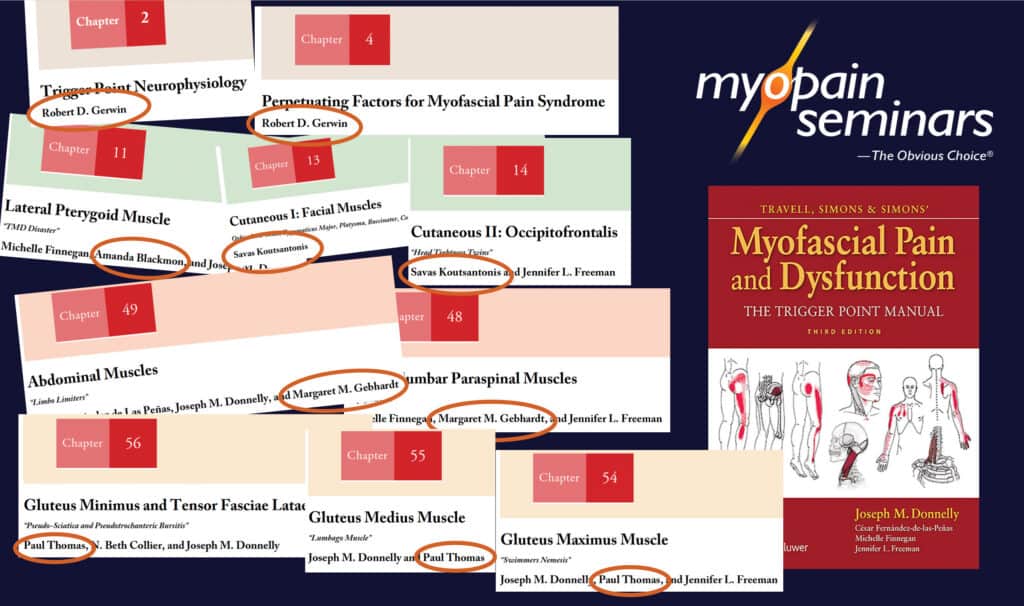
Did you know that many Myopain Seminars instructors have impressive publication records, including important contributions to the last two editions of Travell, Simons, and Simons’ Myofascial Pain and Dysfunction?
Why Many Clinicians Choose Myopain Seminars
Since its founding, Myopain Seminars has emphasized that effective dry needling education must be built on three pillars:
- Scientific evidence
- Clinical reasoning
- Patient safety
Under the leadership of Jan Dommerholt, the company has consistently emphasized anatomy, critical thinking, safety, and integration of dry needling into comprehensive rehabilitation rather than presenting it as a stand-alone technique.
Its faculty includes internationally recognized educators who encourage clinicians not merely to learn procedures but to understand the evidence behind them and develop sound clinical reasoning skills.
The distinction identified by Jenkins et al.—that only one systematic review was judged to have low risk of bias, and that review included Dr. Dommerholt—reinforces the value of learning from educators who actively contribute to advancing high-quality evidence.
The Bottom Line
Evidence-based practice is not simply about reading systematic reviews. It is about critically evaluating how those reviews were conducted. The new Jenkins systematic review reminds us that even publications at the top of the evidence hierarchy deserve careful scrutiny. Of the 38 systematic reviews evaluated, only one met the criteria for low risk of bias.
For clinicians seeking the highest standards in dry needling education, that finding provides another reason to consider learning from leaders who not only teach the evidence but also help create the most methodologically rigorous evidence available. When choosing a dry needling education provider, experience matters.
Teaching matters.
Scientific rigor matters.
And in those areas, Myopain Seminars continues to set the standard.
Jan Dommerholt, PT, DPT | President/CEO, Myopain Seminars
References
1. Jenkins, L., Scanlon, E., Verhagen, A.P., Nasser, A., McCambridge, A., Overton, M., Stubbs, P.W. (2026). Most Systematic Reviews of Dry Needling for Musculoskeletal Pain Have High Risk of Bias: A Systematic Review of Systematic Reviews. JOSPT Methods. Advance publication: https://doi.org/10.2519/josptmethods.2026.0022
2. Pourahmadi M, Dommerholt J, Fernández-de-las-Peñas C, Koes BW, Mohseni-Bandpei MA, Mansournia MA, et al. Dry needling for the treatment of tension-type, cervicogenic, or migraine headaches: a systematic review and meta-analysis. Phys Ther. 2021;101(5).
4. Pourahmadi M, Mohseni-Bandpei MA, Keshtkar A, Koes BW, Fernández-de-las-Peñas C, Dommerholt J, et al. Effectiveness of dry needling for improving pain and disability in adults with tension-type, cervicogenic, or migraine headaches: protocol for a systematic review. Chiropr Man Therap. 2019;27:43.
6. Pourahmadi M, Dommerholt J, Ahmadi M, Schleip R, Farrohi A. Scar Dry Needling Improves Tissue Compliance (Scar-DN): A Randomized Controlled Trial. Under review. 2026.
7. Pourahmadi M, Keshtkar A, Tirotti Saragiotto B, Dommerholt J, Sharma S, Rubinstein SM. The RUnIn Checklist: A Practical Guide for Accurate Reading of Systematic Reviews and Meta-Analyses. Under review.. 2026.