When considering areas for dry needling, anterior hip/groin pain often leads clinicians to target the adductors or hip flexors for local treatment. However, when symptoms are provoked in compressive positions such as flexion, adduction, and internal rotation (FADIR), particularly in weight-bearing, direct needling of the groin likely isn’t getting to the root of the problem. In these cases, the underlying dysfunction may lie in the posterolateral hip rather than the anterior structures.

Dry needling trigger points in the posterolateral hip can improve flexibility and restore neuromuscular efficiency for more optimal mechanics during these tasks. When paired with motor retraining, emphasizing posterior/lateral hip engagement during flexion and internal rotation, patients often observe reduced anterior hip symptoms and improved control.
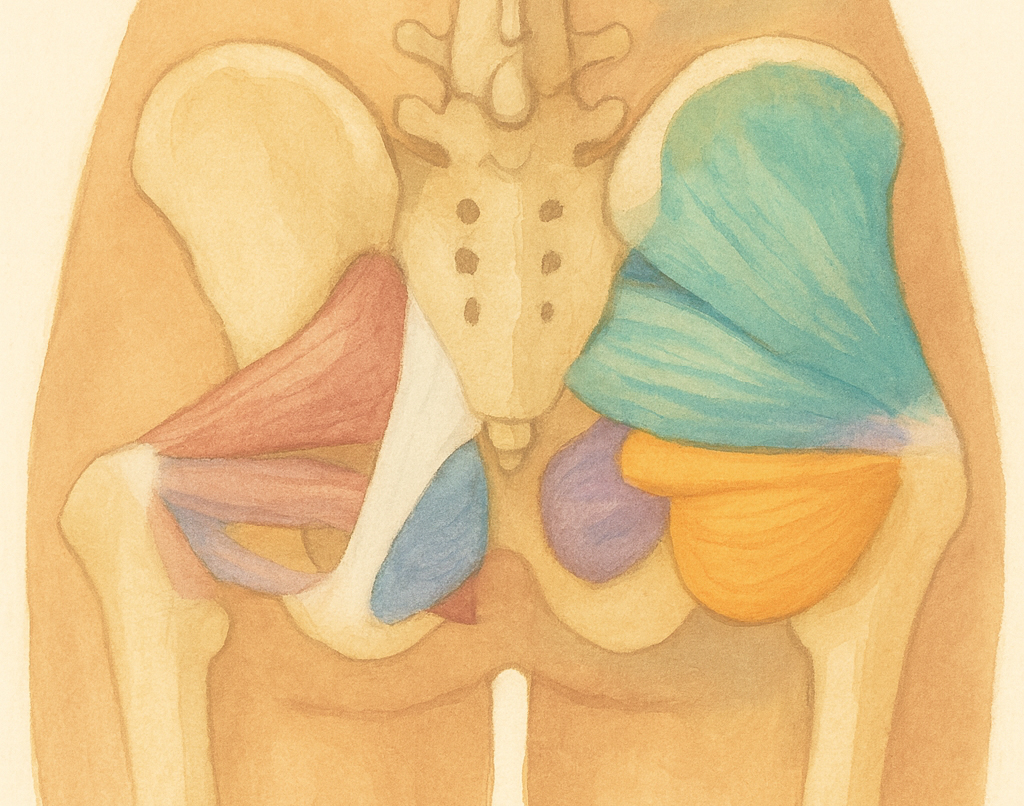
The deep hip rotators, gluteus minimus, and posterior gluteus minimus (to name a few) play a critical role in controlling femoral position during weight-bearing hip flexion and internal rotation. When these muscles are inhibited, inflexible, or laden with trigger points, they may fail to control femoral motion eccentrically. This may lead to excessive anterior and medial glide of the femoral head. This anterior translation increases compressive load on the acetabular rim and surrounding labral and capsular structures, becoming the driving force for this groin pain.
Takeaway: In patients with groin or anterior hip pain reproduced by FADIR testing, consider assessing the posterolateral hip for myofascial dysfunction. Addressing trigger points in this region can offload the anterior capsule, restore balanced joint mechanics, and resolve symptoms that might otherwise persist despite direct treatment of the groin.