
Perhaps it’s simply the clientele I work with, but I’ve seen an increasing number of patients with reverse shoulder replacement surgeries within the last few years. The results have been favorable, particularly for those with significantly arthritic shoulders, severe limited range of motion, function, and pain. Most have regained full, pain-free, and functional range of motion.
The surgery seems simple enough. Replace the deteriorated ball and socket with a reversed ball and socket semiconstrained prosthesis, constructed to stabilize the glenohumeral center of rotation and prevent or minimize superior migration of the humerus.1 Unfortunately, tendons of the rotator cuff and bicep are detached from their distal connections, but the deltoid picks up the slack, compensating for the rotator cuff deficiency. 1
The rehab is relatively straightforward and is usually based on a determined protocol.
The Massachusetts General Hospital Protocol, for example, has five phases:
- Phase I, which occurs 2-3 weeks post-op, requires protection with PROM and no AROM.
- Phase II, during weeks 4-6, requires continued protection but introduces AAROM and progresses to AROM with limitations.
- Phase III, during 7-8 weeks, progresses AROM and some strengthening.
- Phase IV, during 9-11 weeks, includes continued gradual strengthening, and
- Phase V, during 12-16 weeks, involves returning to function.
One of the more common complaints I’ve heard during rehab is anterior shoulder pain. This could, of course, be due to the relocation of the bicep tendon; however, after 8-12 weeks of healing, one would expect the tendon to be scarred down, no longer producing pain, and thus leading to consideration of trigger points. At least that’s where my mind usually goes.
At this point, the most common culprits should be considered, namely the infraspinatus and the deltoid muscles. The infraspinatus muscle is an overworked rotator cuff muscle that is no longer attached but continues to fire. The deltoid is now expected to compensate for a deficiency in the rotator cuff. Checking the pectoralis major and minor, as well as the coracobrachialis, also makes sense, since these muscles are known to refer to the anterior shoulder. And then there are the obscure, maybe less obvious, scaleni and latissimus dorsi muscles.
This is usually the process I run through. However, most recently, after checking off all the boxes listed above, I happened upon the biceps while doing soft tissue work, and there it was! That was my patient’s anterior shoulder pain. The biceps have been shown to contribute to shoulder stability.2 It, along with the rotator cuff, assists in providing glenohumeral joint compression. Further, when the stability of the glenohumeral joint is compromised, the bicep can become weak or overworked.3
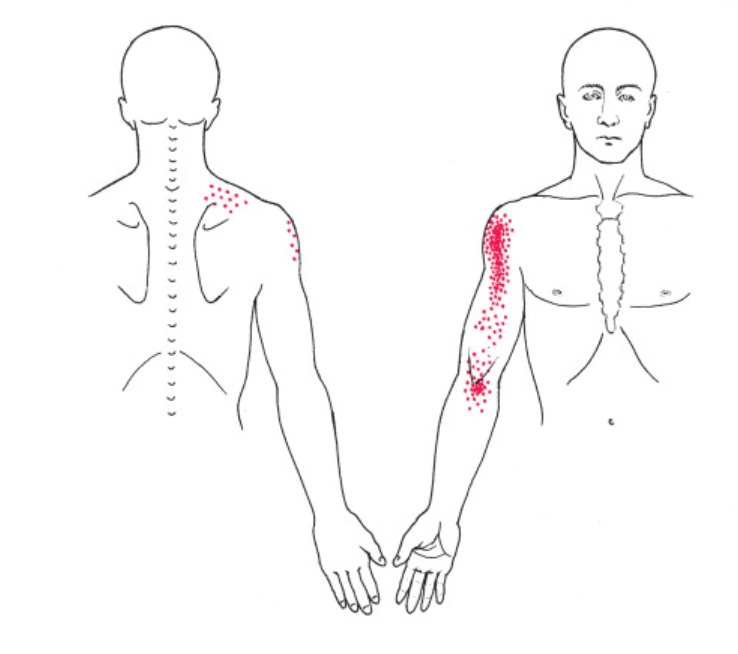
Thanks to Janet Travell, we have referred pain diagrams to guide us in the clinic. I’ve known for years that trigger points can refer sensations other than pain.4 I’ve also known her diagrams represent pain frequency, not pain intensity, meaning the solid red areas are where patients experience pain more often, not necessarily with greater intensity. The speckled or dotted areas indicate where fewer patients experienced pain, regardless of pain intensity. It’s these less frequently referred areas that are often forgotten, which is why I have circled many of them in my resources. And although the anterior shoulder region was colored solid red by Janet Travell, I had not circled it – until now.
Rob Stanborough, PT, DPT, MHSc, MTC, CMTPT, FAAOMPT – Instructor
Just a few references
1Jarrett CD, Brown BT, Schmidt CC. Reverse shoulder arthroplasty. Orthop Clin North Am. 2013;44(3):389-x. doi:10.1016/j.ocl.2013.03.010
2Diplock B, Hing W, Marks D. The long head of biceps at the shoulder: a scoping review. BMC Musculoskelet Disord. 2023;24(1):232. Published 2023 Mar 28. doi:10.1186/s12891-023-06346-5
3Hayes K, Callanan M, Walton J, Paxinos A, Murrell GA. Shoulder instability: management and rehabilitation. J Orthop Sports Phys Ther. 2002;32(10):497-509. doi:10.2519/jospt.2002.32.10.497
4Fernández-de-Las-Peñas C, Dommerholt J. International Consensus on Diagnostic Criteria and Clinical Considerations of Myofascial Trigger Points: A Delphi Study. Pain Med. 2018;19(1):142-150. doi:10.1093/pm/pnx207