
Maria Calatayud-Bonilla PT, PhD, MSc Equine PT – Instructor
When evaluating musculoskeletal dysfunction in horses, it is common to focus on structures such as joints, tendons, or hooves.
Indeed, these are frequent sources of pain and performance limitation. However, in many cases the real cause, trigger points (TrPs) goes unnoticed.
We all know what a TrPs is. We know it is painful upon compression and can evoke characteristic referred pain, motor dysfunction, or autonomic phenomena. In equine practice, TrPs provoke pain and also induce compensatory patterns, stiffness, or even lameness-like symptoms that can easily be mistaken for orthopedic disorders. When these TrPs are not identified, treatment results are often suboptimal, and both practitioners and owners become frustrated with the lack of progress.Many muscles can be affected by TrPs in horses, but three stand out due to their frequency and clinical relevance. Recognizing these “sneaky” trigger points is crucial for improving diagnostic accuracy and therapeutic outcomes.
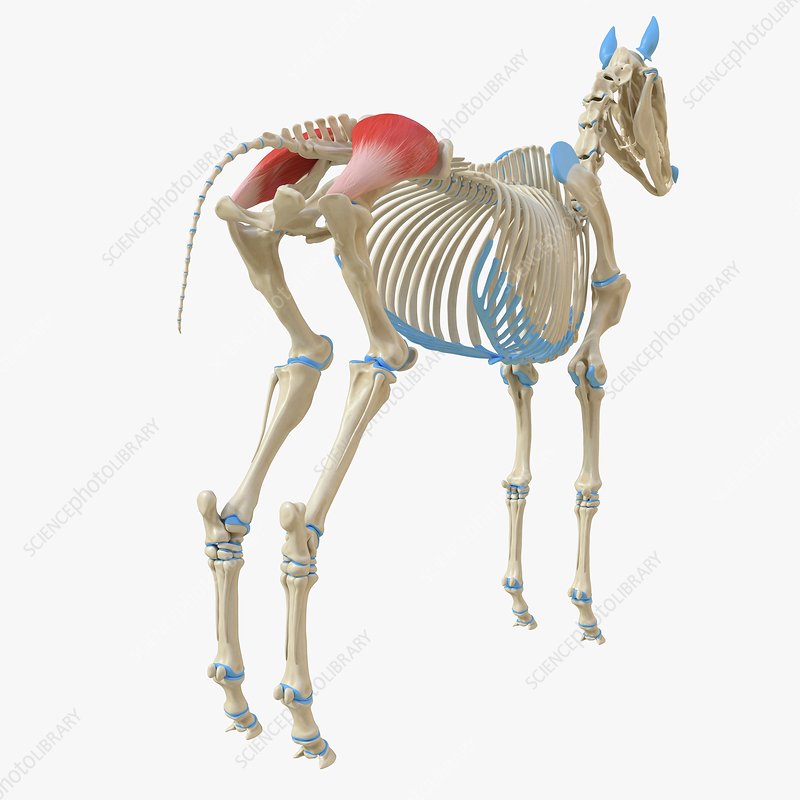
1. Gluteus Medius
The gluteus medius is the largest and most powerful of the gluteal muscles, contributing substantially to propulsion and hindquarter stability. Because of its size and biomechanical role, dysfunction in this muscle has profound consequences.
Typical clinical signs of TrPs in the gluteus medius include:
- Apparent hindlimb lameness without identifiable joint or tendon pathology.
- Difficulty with collection, impulsion, or transitions into canter.
- Tension in lumbar paravertebral muscles, which may limit appropriate movement of the entire back.
- Pain on palpation is often accompanied by local twitch responses or fasciculations.
Clinical relevance: When active TrPs persist, the horse redistributes the workload to synergistic muscles, creating compensatory tension and increasing the risk of secondary dysfunction in the lumbar spine or contralateral limb.
The compensation of a gluteus medius muscle with TrPs can occur ipsilaterally or contralaterally, depending on the function that is lost and the type of movement the horse is trying to maintain.
Ipsilateral: If the right gluteus medius is inhibited, its ipsilateral synergists (biceps femoris, semitendinosus, semimembranosus, gluteus superficialis, and gluteus profundus) may take over its role in hip extension and propulsion.
This leads to overuse and overload of that muscle chain → the horse tends to stiffen the ipsilateral hindquarters.
Contralateral: as a global compensation.
During movements that require pelvic stabilization (transitions, circles, jumping), the contralateral gluteus medius also activates more to balance the pelvis.
The result is an asymmetric propulsion: one side produces the main driving force through its synergist muscles, while the opposite side focuses on stabilizing the pelvis.
This may lead to the horse:
- losing straightness,
- leaning the hindquarters to the affected side,
- showing “false lameness” on the opposite side,
- or placing more weight on the diagonal opposite limb (important at trot).
2. Longissimus Dorsi muscle

Running along the spine, the longissimus dorsi is an extensor of the spine and an essential muscle when transferring hindlimb power forward.
Presentation of TrPs in this muscle often includes:
- Dorsal and lumbar stiffness with reduced flexibility in bending or rounding.
- Poor saddle tolerance, girthiness, or evasive behaviors during tacking.
- Difficulty engaging the back, resulting in a flat or hollow outline under the rider.
Clinical relevance: Such signs are often misinterpreted as primary spinal pathology or even behavioral resistance. Without recognizing the myofascial component, interventions may remain ineffective, while a relatively accessible dysfunction persists untreated.
3. Brachiocephalicus muscle

This long muscle connects the cervical region with the forelimb, playing a role in both head movement and stride length. It is very painful and horses are very reactive to its palpation.
Common findings when TrPs are present include:
- Reduced forelimb protraction and shortened stride.
- Reluctance to stretch forward or downward with the head and neck.
- Subtle gait asymmetries, sometimes interpreted as unilateral forelimb lameness.
Clinical relevance: These horses are often suspected of having primary forelimb pathology or/and cervical issues, such as being reluctant to mantain the neck in several positions and not willing to contact the bit. However, addressing the brachiocephalicus muscle can resolve those issues without unnecessary interventions.
Integrating the Myofascial Assessment into Equine Practice
For professionals, the recognition of myofascial dysfunction is a clinical necessity. Trigger points can alter biomechanics and perpetuate dysfunction if left untreated.
Incorporating systematic palpation and TrPs assessment into every evaluation broadens the differential diagnosis and helps to explain cases that fail to respond to traditional orthopedic or rehabilitation strategies. Moreover, targeted interventions such as dry needling provide a precise and effective way to deactivate TrPs, abolish pain, restore normal muscle function, and improve overall performance.
Final Thoughts
Trigger points in the gluteus medius, longissimus dorsi, and brachiocephalicus are very common. For clinicians, acknowledging their role is essential not only for accurate diagnosis but also for optimizing treatment outcomes. By sharpening our ability to detect these “sneaky” TrPs, we move closer to restoring full function and performance in our equine patients.
References
Bowen, A. G., Goff, L. M., & McGowan, C. M. (2017). Investigation of myofascial trigger points in equine pectoral muscles and girth-aversion behavior. Journal of Equine Veterinary Science, 48, 154-160.
Calatayud-Bonilla, M., Carmona, J. U., & Prades, M. (2025). Clinical Effectiveness of Dry Needling on Myofascial Trigger Points in Horses: A Prospective Algometric Controlled Study. Animals, 15(15), 2207. https://doi.org/10.3390/ani15152207
Macgregor, J., & von Schweinitz, D. G. (2006). Needle electromyographic activity of myofascial trigger points and control sites in equine cleido-brachialis muscle–an observational study. Acupuncture in Medicine, 24(2), 61-70.
Portier, K., Schiesari, C., Gauthier, L., Yeng, L. T., Tabacchi Fantoni, D., & Formenton, M. R. (2025). Comparison of the Prevalence and Location of Trigger Points in Dressage and Show-Jumping Horses. Animals, 15(11), 1558.
Resano-Zuazu, M., Carmona, J. U., & Argüelles, D. (2025). Short-Term Impact of Dry Needling Treatment for Myofascial Pain on Equine Biomechanics Through Artificial Intelligence-Based Gait Analysis. Animals, 15(11), 1517.
Zsoldos, R. R., Voegele, A., Krueger, B., Schroeder, U., Weber, A., & Licka, T. F. (2018). Long-term consistency and location specificity of equine gluteus medius muscle activity during locomotion on the treadmill. BMC veterinary research, 14(1), 126