
Also Known As
“Ten Diagnoses and Not One of Them Correct”
Mary K spent 10 years and $15,000 just trying to tie her shoes without pain.
A decade ago, after crushing it all season on the tennis court, Mary began to experience nagging pain in the front of her shoulder. Her journey, which is not unlike many patients who come to our clinic and seek out dry needling, brought her to the following practitioners:
- Three orthopedic physicians
- Two physiatrists
- Five physical therapists, two of whom were dry needlers
- One acupuncturist
- Two chiropractors
- Three massage therapists
- One occupational therapist
- One Rolfer
- A medicine man energy worker in Sedona
From what she could remember, over the past decade, she has been diagnosed with:
- Supraspinatus tendinitis
- Bicipital tendinitis
- Rotator cuff tendinitis
- Thoracic outlet syndrome
- Cervical radiculopathy
- AC joint dysfunction
- Carpal tunnel syndrome
- Fibromyalgia
- Tennis elbow
- A blocked heart chakra
Her lists of treatments/procedures through the years included:
- Trigger point dry needling
- Cumulative years of physical therapy
- Months of occupational therapy
- EMG/nerve conduction
- Nerve ablations
- Cortisone injections
- Hydro dissection
- Cervical adjustments
- PRP therapy
- Laser therapy
- Past life regression

Mary kept a journal and was very specific with her complaints. Ten years ago, her pain began in the anterior shoulder. As the years progressed, she suffered anterior shoulder pain, and posterior shoulder, forearm and hand pain. Lately, just the extensor forearm and hand hurt and tingled all the time. Gripping things was tough. Tennis was no longer an issue, because she stopped playing it due to pain five years ago. Reaching for and fastening a seatbelt while on the passengers side was excruciating, as was tying her shoe on the opposite side of her body.
Over the past year, she developed an intolerance to bright lights and loud noises and felt like everything aggravated her. She began to think, “maybe this all is in my head,” which is what one of her orthopedic physicians told her after imaging was negative. Hopefully you’re thinking “central sensitization” at this point…
From what I could gather from the interview (and Mary pointing “they always went here, here, and here with dry needles”) it appeared the following muscles were addressed during her years of on-off dry needling sessions:
- Anterior deltoid
- Biceps
- Supraspinatus
- Infraspinatus
- Cervical Multifidi
- Pec Major
- Triceps
- Wrist extensors
Given Mary’s likely mechanism of injury, treatments already tried and failed, history of pain (and evolution into referred pain and central sensitization), can you guess what may have been missed?
HINT:
- The musculocutaneous nerve pierces this muscle
If you guessed coracobrachialis, you are correct.
Often referred to as the “forgotten” muscle, the coracobrachialis can be stressed by things like prolonged slouching (think office workers with poor posture, or kids looking at their cell phones all day), repetitive overhead movements (think tennis and swimming), pushing and pulling (think pull ups and bench press, or that epic “team-building” tug-of-war event).
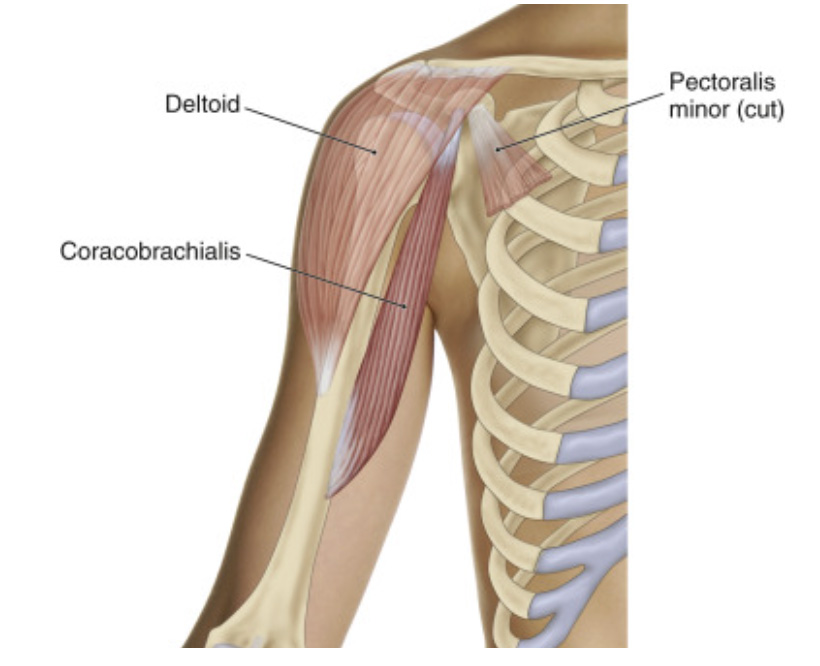
Why do we forget this muscle? For one thing, it’s puny. Our minds tend to gravitate towards looking at the larger, primary drivers of shoulder flexion and shoulder adduction, whereas the coracobrachialis is more like an actor playing a supporting role.
After one session of thoroughly needling the coracobrachialis (along with some synergists), Mary no longer experienced tingling in her forearm and hand. After two sessions, she was clicking a seat belt and tying her opposite shoe without pain, and made a tennis “play date” with her best friend.
When you begin to get your groove with dry needling, people will seek you out. Optimally, this will happen after the patient suffers an acute injury. Unfortunately, the majority of patients come to you after undergoing months, years or even decades of physical therapy and health care procedures that never addressed the problem.
Study your referral patterns, listen to your patient’s subjective tales, know your synergists and antagonists. Remember, it’s rarely the case of “it hurts here, stick a needle here.”
You may just be the one person to help your patient tie her shoes again.